 Microneedling, initially described in 1995, is an aesthetic technique that has re-emerged as a popular alternative in the treatment of acne scarring.1 This technique is gaining more interest, as it is less costly, has minimal downtime, and fewer side effects than other traditional modalities. Acne scarring historically has been a difficult entity to treat for both the physician and the patient, as typically multiple expensive sessions are required with less than optimal outcomes.
Microneedling, initially described in 1995, is an aesthetic technique that has re-emerged as a popular alternative in the treatment of acne scarring.1 This technique is gaining more interest, as it is less costly, has minimal downtime, and fewer side effects than other traditional modalities. Acne scarring historically has been a difficult entity to treat for both the physician and the patient, as typically multiple expensive sessions are required with less than optimal outcomes.
The microneedling technique has been utilized for the treatment of striae, surgical scarring, photoaging, and is now considered a standard treatment for mild (grade I/II) acne scarring.2 A variety of microneedling devices exist with needle sizes ranging from 0.1 mm to 2.5 mm. Outcomes of microneedling vary based on the device, the depth of needle penetration, frequency of needle penetration, and the number of passes.2
The needles traumatically create pores in the dermis, which stimulates the release of growth factors and cytokines. The growth factors and cytokines in turn stimulate collagen, elastin, and neovascularization.3 Studies and case reports have shown that microneedling physically breaks down acne scars and initiates collagen synthesis, specifically collagens I, III, and VII.4 Needling sessions are typically spaced 4 to 6 weeks apart. Microneedling has minimal side effects and can be used safely in patients with skin types I-VI in addition to patients with a history of melasma.3 Microneedling should be avoided in patients with a history of keloid or hypertrophic scarring, inflammatory dermatoses, history of herpes simplex virus in perioral area, or any type of growth in the target area. Absolute contraindications for microneedling include scleroderma, collagen vascular disease, clotting disorders, active infection, and immunosuppression.3
Platelet-rich plasma (PRP) is a highly concentrated autologous serum that is rich in growth factors and cytokines such as platelet-derived growth factor, transforming growth factor, insulin-like growth factor, and vascular endothelial growth factor. These growth factors regulate and induce cell migration, attachment, proliferation, and differentiation as well as promote extracellular matrix accumulation. PRP and the induction of growth factors has been used specifically in the treatment of bony defects, wound healing, gastrointestinal surgery, and more recently in aesthetic dermatology.5
Acne scarring can be categorized by a severity grading scale. Grade I acne scarring is defined as abnormally colored scarring, macular disease. Grade II scarring is mild atrophy or hypertrophy that may only be perceived when <50 cm from the patient. Grade III scarring is moderate atrophic or hypertrophic scars that are not easily camouflaged and can be seen at distances >50 cm. Grade IV is severely abnormally contoured disease that is obvious at social distances, is not easily camouflaged, and cannot be flattened with manual stretching.2
This is a case of microneedling used in conjunction with topical PRP for the treatment of grade II acne scarring.
Read the case on page 2
{{pagebreak}}
Case
A 30-year-old female with no significant past medical history presented to our office with a history of acne in her teens and twenties with grade II acne scarring requesting treatment (Figures 1A-1C). After extensive discussion of other treatment modalities including fractioned laser, chemical peels, and microdermabrasion, the patient decided to try microneedling in conjunction with PRP.
Methods
The treatment, alternatives, and potential risks were discussed with the patient. EMLA cream was used topically to anesthetize the areas of acne scarring. Blood was obtained from the patient using a 10-mL syringe containing acid citrate dextrose. The blood was centrifuged for 10 minutes, separating the PRP from the platelet poor plasma.
The PRP was applied to the areas of scarring immediately prior to and after treatment with the microneedling pen.
The eclipse microneedling device was used at different settings based on anatomic location of the acne scarring with an endpoint of eliciting pinpoint bleeding. On the forehead the needle depth was set to 1.5 mm, the nose and upper lip 1 mm, and on the chin and cheeks 2 mm setting was used.
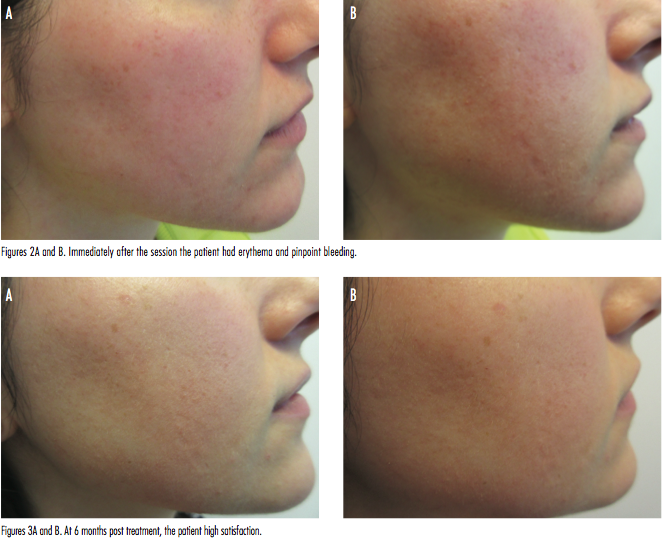
The procedure was well tolerated. Immediately after the session the patient had erythema and pinpoint bleeding (Figures 2A and B). Clinical photos were taken at 1 week and 6 months (Figures 3A and B) after the microneedle session. The patient noted the most significant improvement at 2 months posttreatment session. A scar that can be noted on the right inferior cheek was present since birth.
In our experience, PRP used in conjunction with microneedling for acne scarring has led to more rapid improvement of acne scarring than microneedling alone. A proposed mechanism for this optimal outcome may be that the additional growth factors and cytokines from the PRP act synergistically with the already stimulated neocollagensis secondary to the needling leading to more rapid collagen remodeling. In our patient after 1 session, patient satisfaction was high and scarring was diminished. Larger patient populations with various grades of acne scarring should be studied to further characterize the benefits of PRP with microneedling for acne scarring.
Dr. Lombardi is a fellow at Affiliated Dermatologists in Morristown, NJ.
Dr. Lee is a practicing dermatologist and the director of Procedural Dermatology of the ACGME-approved Procedural Dermatology Fellowship at Affiliated Dermatologists & Dermatologic Surgeons in Morristown, NJ.
Disclosure: The authors report no relevant financial relationships.
References
1. Fernandes D. Minimally invasive percutaneous collagen induction. Oral Maxillofac Surg Clin North Am. 2005;17(1):51-63.
2. Robinson JK, Hanke W, Sigel DM, et al. Surgery of the Skin: Procedural Dermatology. 3rd ed. New York, NY: Elsevier; 2015.
3. Talakoub L, Wesley N. Microneedling. Dermatology News. January 13, 2015. https://www.edermatologynews.com/specialty-focus/aesthetic-dermatology/single-article-page/microneedling/8ba6cca9162ce6bb3ca06fd7fd358dfa.html. Accessed December 31, 2015.
4. El-Domyati M, Barakat M, Awad S, Medhat W, El-Fakahany H, Farag H. Microneedling therapy for atrophic acne scars. J Clin Aesthet Dermatol. 2015;8(7):36-42.
5. Kim DH, Je YJ, Kim CD, et al. Can platelet-rich plasma be used for skin rejuvenation? Evaluation of effects of platelet-rich plasma on human dermal fibroblast. Ann Dermatol. 2011;23(4):424-431.
 Microneedling, initially described in 1995, is an aesthetic technique that has re-emerged as a popular alternative in the treatment of acne scarring.1 This technique is gaining more interest, as it is less costly, has minimal downtime, and fewer side effects than other traditional modalities. Acne scarring historically has been a difficult entity to treat for both the physician and the patient, as typically multiple expensive sessions are required with less than optimal outcomes.
Microneedling, initially described in 1995, is an aesthetic technique that has re-emerged as a popular alternative in the treatment of acne scarring.1 This technique is gaining more interest, as it is less costly, has minimal downtime, and fewer side effects than other traditional modalities. Acne scarring historically has been a difficult entity to treat for both the physician and the patient, as typically multiple expensive sessions are required with less than optimal outcomes.
The microneedling technique has been utilized for the treatment of striae, surgical scarring, photoaging, and is now considered a standard treatment for mild (grade I/II) acne scarring.2 A variety of microneedling devices exist with needle sizes ranging from 0.1 mm to 2.5 mm. Outcomes of microneedling vary based on the device, the depth of needle penetration, frequency of needle penetration, and the number of passes.2
The needles traumatically create pores in the dermis, which stimulates the release of growth factors and cytokines. The growth factors and cytokines in turn stimulate collagen, elastin, and neovascularization.3 Studies and case reports have shown that microneedling physically breaks down acne scars and initiates collagen synthesis, specifically collagens I, III, and VII.4 Needling sessions are typically spaced 4 to 6 weeks apart. Microneedling has minimal side effects and can be used safely in patients with skin types I-VI in addition to patients with a history of melasma.3 Microneedling should be avoided in patients with a history of keloid or hypertrophic scarring, inflammatory dermatoses, history of herpes simplex virus in perioral area, or any type of growth in the target area. Absolute contraindications for microneedling include scleroderma, collagen vascular disease, clotting disorders, active infection, and immunosuppression.3
Platelet-rich plasma (PRP) is a highly concentrated autologous serum that is rich in growth factors and cytokines such as platelet-derived growth factor, transforming growth factor, insulin-like growth factor, and vascular endothelial growth factor. These growth factors regulate and induce cell migration, attachment, proliferation, and differentiation as well as promote extracellular matrix accumulation. PRP and the induction of growth factors has been used specifically in the treatment of bony defects, wound healing, gastrointestinal surgery, and more recently in aesthetic dermatology.5
Acne scarring can be categorized by a severity grading scale. Grade I acne scarring is defined as abnormally colored scarring, macular disease. Grade II scarring is mild atrophy or hypertrophy that may only be perceived when <50 cm from the patient. Grade III scarring is moderate atrophic or hypertrophic scars that are not easily camouflaged and can be seen at distances >50 cm. Grade IV is severely abnormally contoured disease that is obvious at social distances, is not easily camouflaged, and cannot be flattened with manual stretching.2
This is a case of microneedling used in conjunction with topical PRP for the treatment of grade II acne scarring.
Read the case on page 2
{{pagebreak}}
Case
A 30-year-old female with no significant past medical history presented to our office with a history of acne in her teens and twenties with grade II acne scarring requesting treatment (Figures 1A-1C). After extensive discussion of other treatment modalities including fractioned laser, chemical peels, and microdermabrasion, the patient decided to try microneedling in conjunction with PRP.
Methods
The treatment, alternatives, and potential risks were discussed with the patient. EMLA cream was used topically to anesthetize the areas of acne scarring. Blood was obtained from the patient using a 10-mL syringe containing acid citrate dextrose. The blood was centrifuged for 10 minutes, separating the PRP from the platelet poor plasma.
The PRP was applied to the areas of scarring immediately prior to and after treatment with the microneedling pen.
The eclipse microneedling device was used at different settings based on anatomic location of the acne scarring with an endpoint of eliciting pinpoint bleeding. On the forehead the needle depth was set to 1.5 mm, the nose and upper lip 1 mm, and on the chin and cheeks 2 mm setting was used.
The procedure was well tolerated. Immediately after the session the patient had erythema and pinpoint bleeding (Figures 2A and B). Clinical photos were taken at 1 week and 6 months (Figures 3A and B) after the microneedle session. The patient noted the most significant improvement at 2 months posttreatment session. A scar that can be noted on the right inferior cheek was present since birth.
In our experience, PRP used in conjunction with microneedling for acne scarring has led to more rapid improvement of acne scarring than microneedling alone. A proposed mechanism for this optimal outcome may be that the additional growth factors and cytokines from the PRP act synergistically with the already stimulated neocollagensis secondary to the needling leading to more rapid collagen remodeling. In our patient after 1 session, patient satisfaction was high and scarring was diminished. Larger patient populations with various grades of acne scarring should be studied to further characterize the benefits of PRP with microneedling for acne scarring.

Dr. Lombardi is a fellow at Affiliated Dermatologists in Morristown, NJ.
Dr. Lee is a practicing dermatologist and the director of Procedural Dermatology of the ACGME-approved Procedural Dermatology Fellowship at Affiliated Dermatologists & Dermatologic Surgeons in Morristown, NJ.
Disclosure: The authors report no relevant financial relationships.
References
1. Fernandes D. Minimally invasive percutaneous collagen induction. Oral Maxillofac Surg Clin North Am. 2005;17(1):51-63.
2. Robinson JK, Hanke W, Sigel DM, et al. Surgery of the Skin: Procedural Dermatology. 3rd ed. New York, NY: Elsevier; 2015.
3. Talakoub L, Wesley N. Microneedling. Dermatology News. January 13, 2015. https://www.edermatologynews.com/specialty-focus/aesthetic-dermatology/single-article-page/microneedling/8ba6cca9162ce6bb3ca06fd7fd358dfa.html. Accessed December 31, 2015.
4. El-Domyati M, Barakat M, Awad S, Medhat W, El-Fakahany H, Farag H. Microneedling therapy for atrophic acne scars. J Clin Aesthet Dermatol. 2015;8(7):36-42.
5. Kim DH, Je YJ, Kim CD, et al. Can platelet-rich plasma be used for skin rejuvenation? Evaluation of effects of platelet-rich plasma on human dermal fibroblast. Ann Dermatol. 2011;23(4):424-431.
Microneedling, initially described in 1995, is an aesthetic technique that has re-emerged as a popular alternative in the treatment of acne scarring.1 This technique is gaining more interest, as it is less costly, has minimal downtime, and fewer side effects than other traditional modalities. Acne scarring historically has been a difficult entity to treat for both the physician and the patient, as typically multiple expensive sessions are required with less than optimal outcomes.
The microneedling technique has been utilized for the treatment of striae, surgical scarring, photoaging, and is now considered a standard treatment for mild (grade I/II) acne scarring.2 A variety of microneedling devices exist with needle sizes ranging from 0.1 mm to 2.5 mm. Outcomes of microneedling vary based on the device, the depth of needle penetration, frequency of needle penetration, and the number of passes.2
The needles traumatically create pores in the dermis, which stimulates the release of growth factors and cytokines. The growth factors and cytokines in turn stimulate collagen, elastin, and neovascularization.3 Studies and case reports have shown that microneedling physically breaks down acne scars and initiates collagen synthesis, specifically collagens I, III, and VII.4 Needling sessions are typically spaced 4 to 6 weeks apart. Microneedling has minimal side effects and can be used safely in patients with skin types I-VI in addition to patients with a history of melasma.3 Microneedling should be avoided in patients with a history of keloid or hypertrophic scarring, inflammatory dermatoses, history of herpes simplex virus in perioral area, or any type of growth in the target area. Absolute contraindications for microneedling include scleroderma, collagen vascular disease, clotting disorders, active infection, and immunosuppression.3
Platelet-rich plasma (PRP) is a highly concentrated autologous serum that is rich in growth factors and cytokines such as platelet-derived growth factor, transforming growth factor, insulin-like growth factor, and vascular endothelial growth factor. These growth factors regulate and induce cell migration, attachment, proliferation, and differentiation as well as promote extracellular matrix accumulation. PRP and the induction of growth factors has been used specifically in the treatment of bony defects, wound healing, gastrointestinal surgery, and more recently in aesthetic dermatology.5
Acne scarring can be categorized by a severity grading scale. Grade I acne scarring is defined as abnormally colored scarring, macular disease. Grade II scarring is mild atrophy or hypertrophy that may only be perceived when <50 cm from the patient. Grade III scarring is moderate atrophic or hypertrophic scars that are not easily camouflaged and can be seen at distances >50 cm. Grade IV is severely abnormally contoured disease that is obvious at social distances, is not easily camouflaged, and cannot be flattened with manual stretching.2
This is a case of microneedling used in conjunction with topical PRP for the treatment of grade II acne scarring.
Read the case on page 2
{{pagebreak}}
Case
A 30-year-old female with no significant past medical history presented to our office with a history of acne in her teens and twenties with grade II acne scarring requesting treatment (Figures 1A-1C). After extensive discussion of other treatment modalities including fractioned laser, chemical peels, and microdermabrasion, the patient decided to try microneedling in conjunction with PRP.
Methods
The treatment, alternatives, and potential risks were discussed with the patient. EMLA cream was used topically to anesthetize the areas of acne scarring. Blood was obtained from the patient using a 10-mL syringe containing acid citrate dextrose. The blood was centrifuged for 10 minutes, separating the PRP from the platelet poor plasma.
The PRP was applied to the areas of scarring immediately prior to and after treatment with the microneedling pen.
The eclipse microneedling device was used at different settings based on anatomic location of the acne scarring with an endpoint of eliciting pinpoint bleeding. On the forehead the needle depth was set to 1.5 mm, the nose and upper lip 1 mm, and on the chin and cheeks 2 mm setting was used.
The procedure was well tolerated. Immediately after the session the patient had erythema and pinpoint bleeding (Figures 2A and B). Clinical photos were taken at 1 week and 6 months (Figures 3A and B) after the microneedle session. The patient noted the most significant improvement at 2 months posttreatment session. A scar that can be noted on the right inferior cheek was present since birth.
In our experience, PRP used in conjunction with microneedling for acne scarring has led to more rapid improvement of acne scarring than microneedling alone. A proposed mechanism for this optimal outcome may be that the additional growth factors and cytokines from the PRP act synergistically with the already stimulated neocollagensis secondary to the needling leading to more rapid collagen remodeling. In our patient after 1 session, patient satisfaction was high and scarring was diminished. Larger patient populations with various grades of acne scarring should be studied to further characterize the benefits of PRP with microneedling for acne scarring.
Dr. Lombardi is a fellow at Affiliated Dermatologists in Morristown, NJ.
Dr. Lee is a practicing dermatologist and the director of Procedural Dermatology of the ACGME-approved Procedural Dermatology Fellowship at Affiliated Dermatologists & Dermatologic Surgeons in Morristown, NJ.
Disclosure: The authors report no relevant financial relationships.
References
1. Fernandes D. Minimally invasive percutaneous collagen induction. Oral Maxillofac Surg Clin North Am. 2005;17(1):51-63.
2. Robinson JK, Hanke W, Sigel DM, et al. Surgery of the Skin: Procedural Dermatology. 3rd ed. New York, NY: Elsevier; 2015.
3. Talakoub L, Wesley N. Microneedling. Dermatology News. January 13, 2015. https://www.edermatologynews.com/specialty-focus/aesthetic-dermatology/single-article-page/microneedling/8ba6cca9162ce6bb3ca06fd7fd358dfa.html. Accessed December 31, 2015.
4. El-Domyati M, Barakat M, Awad S, Medhat W, El-Fakahany H, Farag H. Microneedling therapy for atrophic acne scars. J Clin Aesthet Dermatol. 2015;8(7):36-42.
5. Kim DH, Je YJ, Kim CD, et al. Can platelet-rich plasma be used for skin rejuvenation? Evaluation of effects of platelet-rich plasma on human dermal fibroblast. Ann Dermatol. 2011;23(4):424-431.
















